An informatics tool to analyse child growth indexes: first results of Mid-Upper Arm Circumference (MUAC) software
Andrea Malizia,1 Stefania Moramarco,1 Riccardo Rossi,2 Paola Scarcella,1 Pasqualino Gaudio,2 Leonardo Palombi1 and Ersilia Buonomo1
Department of Biomedicine and Prevention, University of Rome “Tor Vergata”, Rome, Italy
Department of Industrial Engineering, University of Rome Tor Vergata, Rome, Italy
Introduction
Growth monitoring is a widespread public health practice for both prevention and treatment of child malnutrition. Paediatric centres use the growth chart to check child health and development, both in routine maternal and child health services and in specific nutritional rehabilitation programs.1 Several pathologies and diseases have a negative impact on growth indexes and influence the child growth velocity.2 Therefore, its measurement can be used to monitor, prevent or mitigate various health problematics in children.3 The World Health Organization (WHO) fixed several growth indexes. Three indexes describe the growth velocity: weight, length and head circumference velocities. Moreover, there are indexes those describe the mean value for age: height for age, weight for age, body mass index for age, head circumference for age, arm circumference for age, subscapular skinfold for age and triceps skinfold for age. Finally, weight for length is also largely used.4,5,6 Growth indexes are strongly influenced by child nutrition. It is an evidence that child malnutrition is one of the most crucial child problematics. It increases the risk of chronical illness, social isolation, morbidity, poor neurodevelopment, depression and many others.7,8 Furthermore, malnutrition is a health problem worldwide spread. Undernutrition mainly threats low-middle income countries and some developed countries where there are groups with large socio-economic inequalities.9,10 Contrariwise, obesity and overweight are diffused in middle and high-income countries.11
A software tool able to analyse malnutrition index as MUAC in children represents an important contribution for children malnutrition surveillance system to reach the sustainable goal number 2 “zero hunger”.12
The development of software tools to analyse child growth indexes could be useful to enhance child health monitoring system, improving statistical analysis and discovering correlations between anthropometric indexes and diseases. The department of Biomedicine and Prevention and the department of Industrial Engineering of the University of Rome “Tor Vergata” are joining the forces to develop software tools able to perform data statistical analyses of the indexes in very short time. These tools will be able to analyse any growth index following the WHO standards. It will be designed to have a friendly user interface and it will be distributed to the scientific and medical community.
In this work, the authors show a software to analyse the Mid-Upper Arm Circumference (MUAC). MUAC is the measurement of left upper arm, taken at the mid-point between the tips of the shoulder and the tips of the elbow. It is an indicator widely used to early identify children at high risk of death in case of malnutrition and their response to nutritional rehabilitation.13,14,15 Therefore, MUAC is largely used as a screening measurement tool in community-based nutrition programs.16
Many softwares already give the possibility to analyse MUAC from database or single patient. Anyway, the novelty of this work lies in the software features and its entirety. Because of that, at the end of the paper we will describe, in brief, the main differences between the existing software and the new one developed.
Software features and algorithms
The tool is developed under the programming environment of LabVIEW – National Instrument (NI). LabVIEW is a visual programming language composed by two different structures, the block diagram and the front panel. The block diagram is the core of the algorithms of the software (Figure 1) while the front panel is the user interface. The authors developed the tool in LabVIEW because it has an easy to use application builder tool to turn the code in an .exe distributable file that can be installed also in PC without the NI platform and a customisable user interface that can be modified easily also from non-experts in programming. In fact, one of the most important features we want to achieve with this work is the easiness of the software. It has to extract many information with small computational time and in easy ways.
Figure 1. One part of the software block diagram. In this section, the software computes the z_score through the standard statistical parameters (L, M and S) and MUAC value (y).
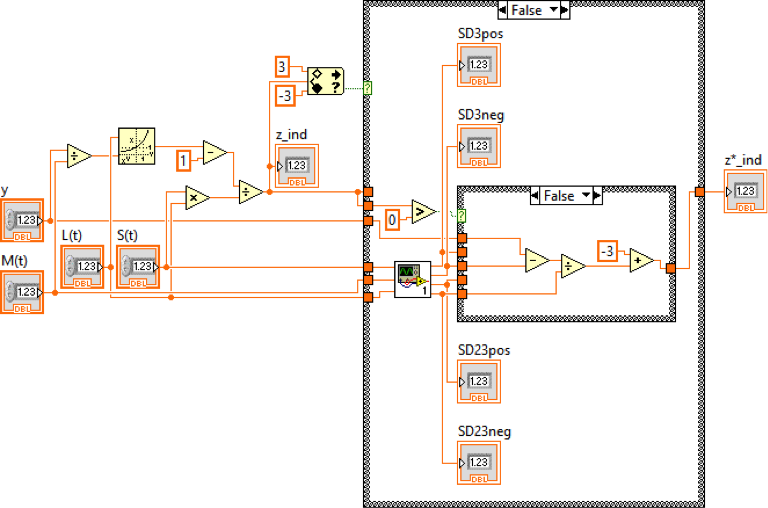
Figure 1 shows a limited part of the software block diagram. Inputs, outputs and functions are linked through virtual wires. In the figure is represented the code about the computation of the Z-scores of the MUAC for age, usually called ZMUAC. It is an important parameter, since it expresses how standard deviation the analysed value is far from the standard population.
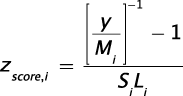
Each analysis is performed following the standards given by the WHO. The MUAC standards are divided in two classes, for males and females. The values are given each day from the 91st day of life (3 months) to the 1856th (5 years). The tool is able to compute statistical analyses reading the patient information. The necessary inputs for each patient are the identification code, birth date, medical examination date and MUAC value. Firstly, the software load the data stored in a .txt, .csv or .xls file. Then, it iteratively computes each patient. The male and female indicators inputs allow to choice the right standard values. The birth and medical examination dates are converted from strings to timestamps variables. Timestamps is a sequence of character that allows to make operation on dates. Subtraction between medical examination and birth timestamps gives the seconds of life. Dividing it by the seconds in a day, the software computes days of life. Therefore, the software looks for the L, M and S values referred to the days of life. Then, the child zscore is computed through the following equation (1):
The LMS methods requires a correction of z_score when its absolute value exceeds three. The correction is reached through the following equations (2-6):
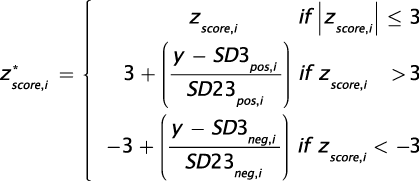




The z*score is the correct z-score of the patient analyzed. Figure 2 shows the user interface that has been built to be as easy as possible. The software functioning requires to the user only few steps. Firstly, it must have the patient to analyze in the following format:
Figure 2. User interface of the software
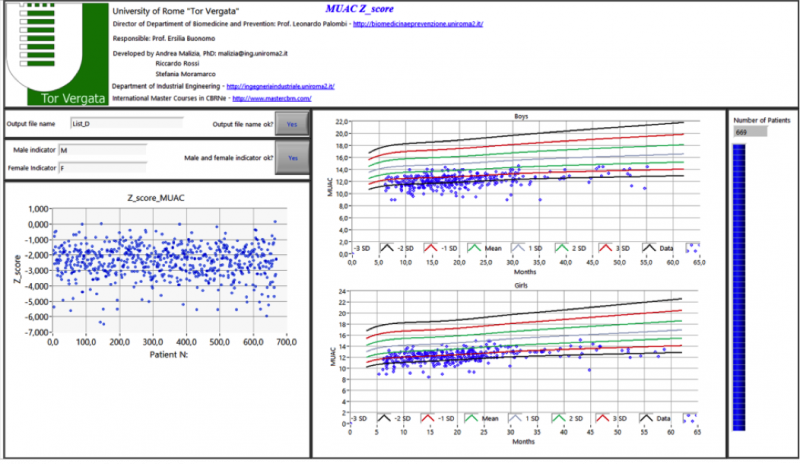
Table 1. Input file format: the first row contains the labels. The other rows describe the patients to analyze.

When the software starts, user must select the file path of children to analyze. Then, a pop-up requires the user to select where the output files must be saved. In the interface panel, user has to type the name of output files. Then, it has to write how male and female indicators are written in the input file. For example, if the gender is indicated through “boy” and “girl” string, the user must type “boy” and “girl” in the male and female indicator inputs. Then, it can press the two bottoms (Figure 3).
Figure 3. Required inputs: Output file name, male (M) and female (F) indicators and buttons to start the computation.
Two flagging rules are implemented to give information about the health of patients. The first is based on MUAC value. According to the International Guidelines, if the MUAC is lower than 12.5 cm the patient is considered in warning condition (affected by moderate acute malnutrition); if the MUAC is lower than 11.5 cm, the patient health is critical (affected by severe acute malnutrition).17 A second flagging rule is obtained through the ZMUAC. A ZMUAC lower than -2 is considered in warning condition while lower than -3 is critical. The presence of edema is considered in the warning rules. Then, if the patient is affected by edema, the condition is considered critical, independently from ZMUAC and MUAC values. Warnings are given both in the main output file (Table 2) and in a separated file where all the patients in critical and warning condition are recorded. Therefore, the software starts the analysis. The outputs are one .txt file and several graphs. The .txt file has the following format:
Table 2. Output file format (.txt). In the first five columns, it returns the same input variables while in the sixth it writes the z_score.

The tool also creates five images those show some statistics of the analyzed children.
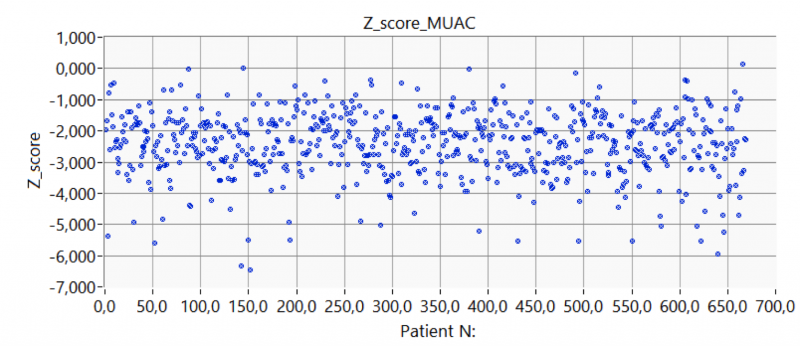
A scatterplot is made placing in the x-axis the patient number (1 is the first patient analyzed and so on), while the y-axis shows the correlated z_score values. It allows to see if there are critical z_score and identify the patient.
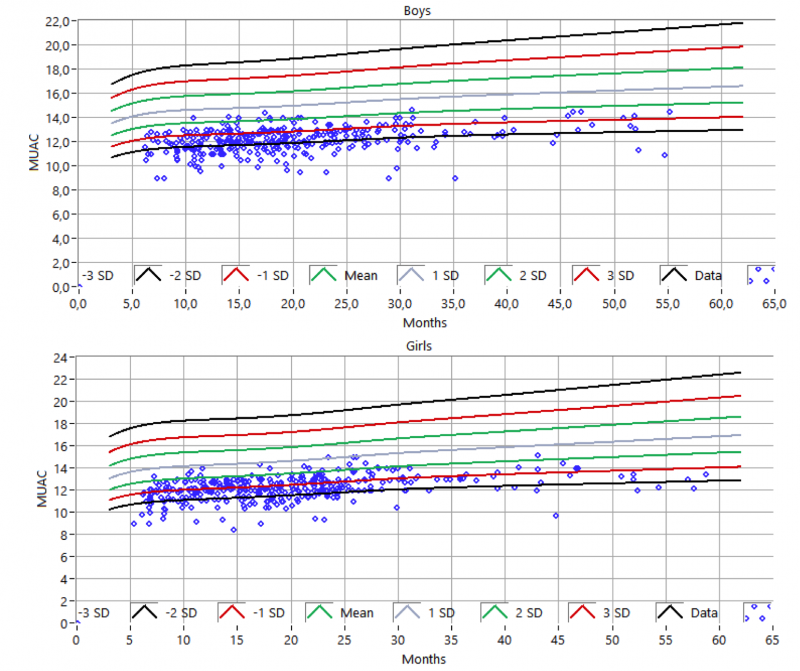
Other two graphs represent scatterplots with lines that represent the values of WHO standards. The graphs are divided into boys and girls since the standards are different. They allow to evaluate graphically how each child is away from the WHO standards and identify what are the children with most critical values.
A second graph shows the comparison of the standard distribution between the sample and the WHO standards. For each patient, the software correlates the standard values that the patient should have. Therefore, mean and standard deviation of sample and WHO standard value are computed. Then, the standard distributions are drawn through the statistical properties (mean and standard deviation). This graph allows to understand how the sample is different from the mean and standard deviation of the standard values.
A cumulative distribution in function of z_score is also performed. The cumulative frequency is performed through the following equation (7):

Where:
- Fi : cumulative frequency for the interval i;
- Fi-1 : cumulative frequency in the interval i-1;
- Δi : interval amplitude.
Since the cumulative frequency represents the integral of standard distribution, the maximum value is one. It gives the probability to obtain a z-score lower (or higher) than a certain value.
The entire graphs are both shown in the user interface and saved in the output folder selected by the user.
The blue filling bar at the right of the user interface shows the ratio between data analyzed and all input data. Therefore, it represents the status of the computation and its speed.
Results
In this section, the authors show the results about a sample of malnourished children and each correlated graph. Then, they validate the software using MUAC values that match to two percentiles.
Figure 4 shows the scatter plot of z_score. It is clear that these values represent children affected by malnutrition. While there are many patients those can be considered in healthy conditions, some children have a very low z_score, lower than -5. These values could imply severe or critical conditions.
Figure 4. Sample distribution compared with the standard distribution.
The software is able also to compare sample and standard distributions. The sample mean is largely lower than the standard distribution, indices that the sample could be affected by growth problematics. Furthermore, the sample distribution is shorter and wider, that implies a large variability of the sample. The large wide suggests that could be there some child with very low MUAC values.
The software can calculate also the cumulative frequency calculating the probability to find a child with a z_score lower than a certain value. The 50% of the children has a z_score lower than -2.5 that advises again the presence of large growth problematics. Furthermore, the 100% is reached before than z_score equal to zero. It suggests that all the sample is deviated to lower MUAC values. Moreover, the 10% of children have a z_score lower than -4, it could imply severe acute malnutrition of these, and fast interventions could be needed.
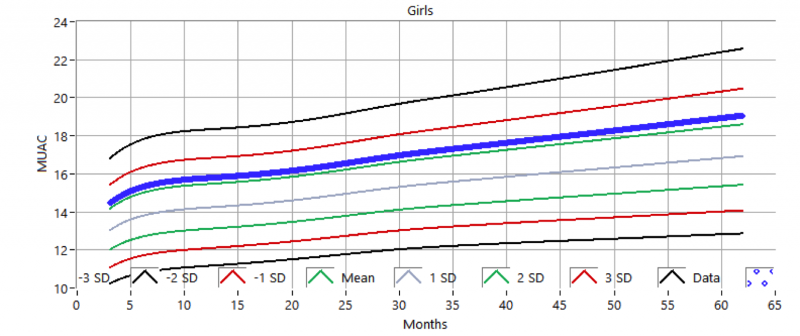
Figure 5 shows the comparison between MUAC of the sample and standard deviation lines of the standard models. The graphs are divided in two graphs, since the models are two, one for males and one for females. These two graphs are useful to understand if a child is away from the standard models and quantify this distance. The grey line in the middle represents the mean values of standard distribution. Mean is the ideal value that a child should have. Then, green lines represent one standard deviation from the mean, red lines are two standard deviations and black lines are three. Therefore, child could have malnutrition problem as far the child MUAC is far from mean values.
Figure 5. Analyzed MUAC compared with the mean and standard deviation of the standard distribution (boys and girl).
In this case, the software has computed the analysis of 669 children in less than 15 seconds.
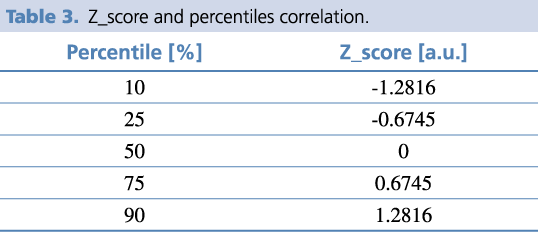
In order to validate the tool, the software has been tried with two samples of patients. The first data is compounded by only male patients with MUAC values equal to the 25th percentiles of the standard deviation. The second sample are only females with MUAC values of the 90th percentiles. These values are taken from the WHO site. The size of samples is 1766 patients, one for days of life. These go from 91 to 1856 days. Therefore, gender detection, days of life calculation and z_score evaluation can be validated through these two analysis. In the standard distribution, one z_score value matches to only one percentile. The following table shows some percentile – z_score correspondence.
Table 3. Z_score and percentiles correlation.
The first sample is male with MUAC in the 25th percentile region. Figure 6 shows the scatter plot of these data. All the data points have one z_score value that matches with the 25th percentiles (z_score = -0.6745). The values have not oscillations or values outside from the proper value. It means that z_score computation works well and never wrong.
Figure 6. Z_score of first test sample (25th percentile - males): the z-score is constant and equal to -0.6745.
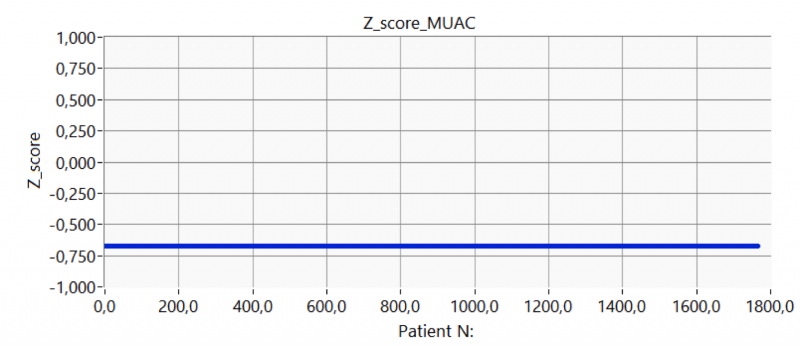
Figure 7 shows the MUAC values compared the mean and standard deviation lines. Obviously, the MUAC values follow the line shape and it is included inside the one standard deviation region.
Figure 7. Analyzed male MUAC of 25th percentile compared with the mean and standard deviation of the standard distribution.
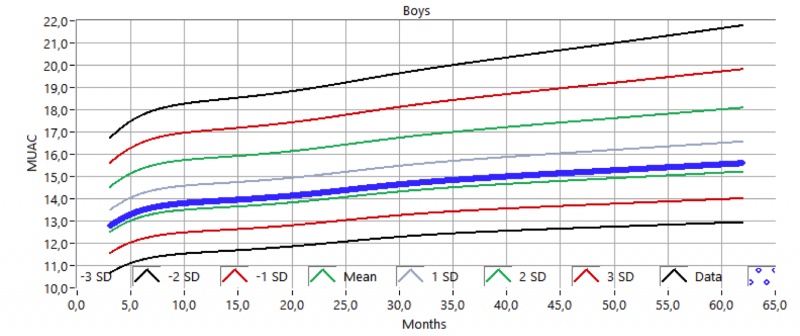
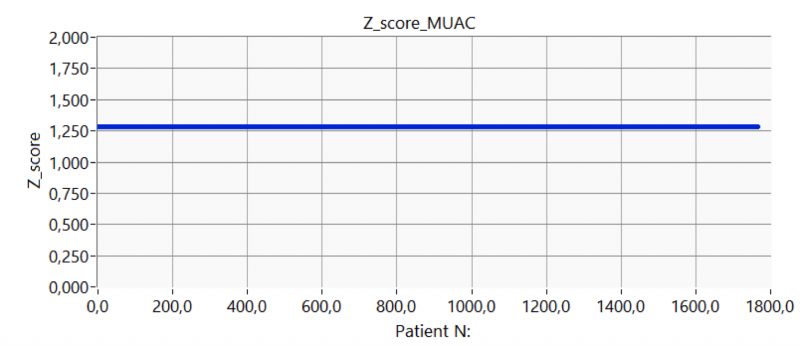
Figure 8 shows the scatter plot of the second test sample. The z_score values match with the expected ones also in this case. The z_score values are constants and equals to the value of the 90th percentiles.
Figure 8. Z_score of first test sample (90th percentile – female): the z-score is constant and equal to 1.2816.
The comparison between the second test sample and standard deviation lines is shown in Figure 9. Accordance between results and expectations is again reached.
Figure 9. Analyzed female MUACs of 90th percentile compared with the mean and standard deviation of the standard distribution.
In these tests, standard distribution comparison and cumulative frequency are not shown because they not make relevant results to validate the software since standard deviation comparisons show the comparison between mean and 25th (or 90th) percentile while the cumulative frequency is a vertical line. The analysis of the 1766 patients is very short (< 30 seconds).
The results about software validation clearly show the aptitude of the software to compute statistical analysis of large data in short time. The absence of oscillations in the scatter plot confirms a good accuracy of the software.
A computational time analysis has been performed using a large number of sample data. The computational time is about 0.1 ms per patient.
In this last part of the paper the authors report a comparison of the features of the developed software with the one already existing. This comparison is done with the most used tools:
- WHO Anthro is mainly an individual anthropometric calculator, i.e. it analyses patient per patient. Our software computes data with large numbers of patients.
- ENA for SMART is another important software in malnutrition fields. ENA for SMART provides analyses per gender and age, but not for gender and age at the same time.
- Epiinfo7 is not provided by MUAC and ZMUAC analyses.
- In case of R, SAS, S-Plus, SPSS and STATA scripts, the major issues are related to the fact that these are not user-friendly interfaces for these software, which usually led to several difficulties for people not particularly able in programming and software usages.
Conclusion
The growth parameters are useful indexes for child growth surveillance, to determine child malnutrition and other correlated medical problems and to monitor the response to treatments and therapies. The World Health Organization has developed a standard statistical model, used worldwide, to analyse data. There are several growth parameters and the correlation between these parameters and certain medical conditions is still a key point for research activities. In order to develop properly these analysis is fundamental to compute and elaborate huge amount of data coming from field database in order to improve robust statistical analysis. Therefore, it is essential to provide the scientific community with user-friendly tools able to give accurate and complete data set in short time.
In this work, the authors present main tool features. The software is able to computes the z_score of MUAC, taking as inputs the identification code, the birth date, the examination date, the gender and the MUAC values. Besides the data file, the tool has graphical outputs: scatterplots, standard distribution comparison, cumulative frequency and data comparison with standard values. All these graphs give the needed information to understand if the sample has or not healthy values.
The authors tested the software with a significant sample of malnourished children. The analysis of the results shows the low values of MUAC and z_score. The cumulative frequency shows a large percentage of children with a z_score lower than -3 and also the comparison of the standard distributions demonstrates a large shift of MUAC on the low values area. The data compared with standard deviation lines show immediately the large number of children with very low MUAC values. Therefore, it is clear that the sample contains several patients with growth failure issues, in this case linked to malnutrition. The analysed sample contained 669 patients. The software computed the analysis in very short time (<15 seconds). The software has been tried with two test samples with which the statistical analyses are known (25th and 90th percentiles showing its ability to compute accurate statistical analysis.
Acknowledgments
The activity mentioned in the paper is under the scientific umbrella of the research program DREAM. Here the description of the program taken from Wikipedia:
(https://en.wikipedia.org/wiki/Drug_Resource_Enhancement_against_Aids_and_Malnutrition)
“DREAM (short for “Drug Resources Enhancement against Aids and Malnutrition”, formerly “Drug Resource Enhancement against AIDS in Mozambique”) is an AIDS therapy program promoted by the Christian Community of Sant’ Egidio. It is designed to give access to free ARV treatment with generic HAART drugs to the poor in Africa on a large scale: So far, 5,000 people are receiving ARV treatment, especially in Mozambique, but the program is being built up also in other countries: Malawi, Guinea, Tanzania and others. Despite being free, the program aims at excellence in treatment, providing the best existent range of drugs (HAART) and regular blood testing according to European standards. It is linked with a nutrition program as well as guidance and sanitary education by volunteers (other HIV patients taking part in the program), which encourages new patients to comply and come to the appointments. The compliance rate is very high (94 percent).”
The scientific responsible of the program is Prof. Leonardo Palombi.
References
- E. Buonomo, S. De Luca, D. Tembo, P. Scarcella, P. Germano, A.M. Doro Altan, L. Palombi, G. Liotta, K. Nielsen-Saines, F. Erba, M.C. Marrazzi, Nutritional Rehabilitation of HIV-Exposed Infants in Malawi: Results from the Drug Resources Enhancement Against AIDS and Malnutrition Program, Int J Environ Res Public Health. 9(2) (2012) 421–434. doi:10.3390/ijerph9020421.
- E. Buonomo, P. Scarcella, D. Tembo, M. Giuliano, S. Moramarco, L. Palombi, K. Nielsen-Saines, S. Mancinelli, M.C. Marazzi, Malnutrition Decreases the Odds of Attaining Motor Milestones in HIV Exposed Children: Results from a Paediatric DREAM Cohort. Epidemiol. Prev. 39(4 Suppl 1) (2015) 108-12.
- M. K. Mwangome, G. Fegan, T. Fulford, A. M. Prentice e J. A. Berkley, Mid-Upper Arm Circumference at Age of Routine Infant Vaccination to Identify Infants at Elevated Risk of Death: A Retrospective Cohort Study in the Gambia, Bull. World Health Organ. 90 (2012) 887-894. doi: 10.2471/BLT.12.109009.
- WHO Multicentre Growth Reference Study Group, WHO Child Growth Standards: Length/Height-For-Age, Weight-For-Age, Weight-For-Length, Weight-For-Height and Body Mass Index-For-Age: Methods and Development. http://www.who.int/childgrowth/standards/technical_report/en/, 2006 (accessed 03.04.2017)
- WHO Multicentre Growth Reference Study Group, WHO Child Growth Standards: Head Circumference-For-Age, Arm Circumference-For-Age, Triceps Skinfold-For-Age and Subscapular Skinfold-For-Age: Methods and Development. http://www.who.int/childgrowth/standards/second_set/technical_report_2/en/ , 2007 (accessed 15.03.2017)
- WHO Multicentre Growth Reference Study Group, WHO Child Growth Standards: Growth Velocity Based on Weight, Length and Head Circumference: Methods and Development. http://www.who.int/childgrowth/standards/velocity/technical_report/en/ , 2009 (accessed 12.04.2017)
- L. S. Adair e et al., Associations of Linear Growth and Relative Weight Gain During Early Life with Adult Health and Human Capital in Countries of Low and Middle Income: Findings from Five Birth Cohort Studies, Lancet. 382(9891) (2013) 525-34. doi: 10.1016/S0140-6736(13)60103-8
- P. Scarcella, S. Moramarco, E. Buonomo, K. Nielsen-Saines, H. Jere, G. Guidotti, L. Palombi, M. C. Marazzi, The Impact of Malaria on Child Growth: Anthropometric Outcomes in a Pediatric HIV-Exposed Cohort in Malawi. Biomedicine & Prevention 2016. Cohort Studies, Biomed. Prev. 1 (53) (2016). doi:10.19252/000000035
- L. D. Howe, K. Tiling, B. Galobardes, G. D. Smith, D. Gunnell e D. A. Lawlor, Socioeconomic Differences in Childhood Growth Trajectories: at What Age Do Height Inequalities Emerge? J. Epidemiol. Commmunity Health, 66 (2), (2010) 143-148. doi: 10.1136/jech.2010.113068
- L. Fairley, E. S. Petherick, L. D. Howe, K. Tilling, N. Cameron, D. A. Lawlor, J. West e J. Wright, Describing Differences in Weight and Length Growth Trajectories between White and Pakistani Infants in the UK: Analysis of the Born in Bradford Birth Cohort Study Using Multilevel Linear Spline Models, Arch. Dis. Child., 98 (4), (2013) 274-279. doi: 10.1136/archdischild-2012-302778
- S. Gallus, A. Lugo, B. Murisic, C. Bosetti, P. Boffetta e C. La Vecchia, Overweight and Obesity in 16 European Countries, Eur. J. Nutr. 54 (5) (2015) 679-689. doi: 10.1007/s00394-014-0746-4
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. (2015). https://sustainabledevelopment.un.org/content/documents/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf
- A. Briend e et al., Low Mid-Upper Arm Circumference Identifies Children with a High Risk of Death Who Should Be the Priority Target for Treatment, BMC Nutrition. 2 (63) (2016). http://dx.doi.org/10.1186/s40795-016-0101-7
- P. J. Binns, N. M. Dale, T. Banda, C. Banda, B. Shaba, M. Myatt, Safety and Practicability of Using Mid-Upper Arm Circumference as a Discharge Criterion in Community Based Management of Severe Acute Malnutrition in Children Aged 6 To 59 Months Programmes, Arch. Public Health. 74 (24) (2016). doi: 10.1186/s13690-016-0136-x
- S. Moramarco, G. Amerio, L. Chafula Muyaba, D. Bonvecchio, E. Abramo, L. Palombi, E. Buonomo, Nutritional Counseling Improves Dietary Diversity and Feeding Habits of Zambian Malnourished Children Admitted in Rainbow Nutritional Programs, Biomedicine and Prevention. 1 (2017) 666. DOI:10.19252/00000005D
- S. Moramarco, G. Amerio, C. Ciarlantini, J. Kasengele Chipoma, M. Kakungu Simpungwe, K. Nielsen-Saines, L. Palombi, E. Buonomo, Community-Based Management of Child Malnutrition in Zambia: HIV/AIDS Infection and Other Risk Factors on Child Survival, Int. J. Environ. Res. Public Health. 13(7) (2016) 666. doi: 10.3390/ijerph13070666
- World Health Organization, United Nations Children’s Fund. Child Growth Standard and Identification of Severe Acute Malnutrition in Infant and Children. A Joint Statement; WHO: Geneva, Switzerland. (2009). http://apps.who.int/iris/bitstream/10665/44129/1/9789241598163_eng.pdf?ua=1 (accessed 19.10.2017)